It began with a just a handful of cases in Guinea in March. But it
spread quickly to two other countries and is now the deadliest outbreak
of Ebola virus on record.
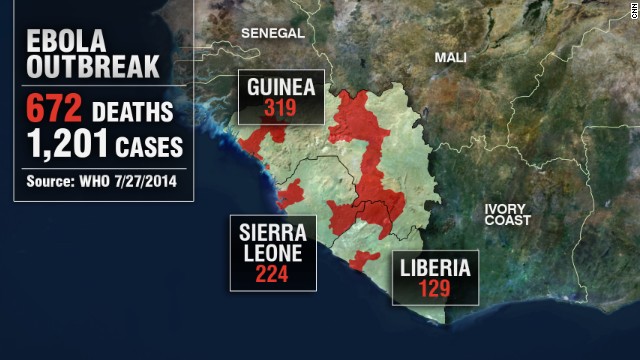
At least 1,201 people in
Guinea, Sierra Leone and Liberia have been infected by what is believed
to be Ebola virus since its symptoms were first observed in March,
according to the World Health Organization. 672 of them have died. That's a 55% percent mortality rate.
The WHO says "drastic
action is needed" to contain Ebola, which has spread from rural areas to
cities in West Africa and sparked fears that the killer virus could
spread to other continents.
What's the latest?
Until recently the Ebola
outbreak had been contained to three West African countries: Guinea,
where it began, Liberia and Sierra Leone.
But this week a Liberian government official who had contracted the virus
died in isolation at a hospital in Lagos, Nigeria.
 Photos: Ebola outbreak in West Africa
Photos: Ebola outbreak in West Africa
 Ebola outbreak kills an American
Ebola outbreak kills an American
 Fighting Ebola on the front lines
Fighting Ebola on the front lines
 American doctor battling Ebola
American doctor battling Ebola
Patrick Sawyer,
a naturalized American citizen who worked in Liberia, had stopped in
Nigeria for a conference but died before he could board a plane home to
the U.S. He's the first American to die in the latest outbreak, though
several other U.S. aid workers in Liberia have also contracted Ebola and
are being treated.
Why was someone infected with Ebola allowed on a plane?
It is unknown whether
Sawyer was displaying symptoms of Ebola before he flew from Monrovia,
Liberia's capital, to Ghana and then to Togo to switch planes to fly to
Lagos. His Minnesota-based widow, Decontee Sawyer, told CNN that he had
cared for his Ebola-stricken sister in Liberia, though she said he
didn't know at the time that she had the virus. When he arrived in
Nigeria he told officials that he had no direct contact with anyone who
had Ebola.
But since it takes
between 2 and 21 days before someone infected with Ebola begins to show
symptoms, there's little health officials can do to stop an infected but
non-symptomatic person from flying to another country,
said CNN's Chief Medical Correspondent Sanjay Gupta.
"When I left Conakry
(Guinea's capital), they took my temperature at the airport and asked me
to fill out a questionnaire, and that was really about it," said Gupta.
"If I had been exposed for whatever reason and it was 21 days later
before I got sick, there was nothing that would have prevented me from
getting on that plane.
"I think it's going to
happen at some point. Just from observing the whole process it's almost
impossible from happening," Gupta said, before adding that he believes
the virus would stand little chance of spreading very far in a developed
country.
How easily could Ebola spread on a plane?
Serious viruses like Ebola may be just "a plane ride away" from reaching the developed world, according to
Marty Cetron of the Centers for Disease Control and Prevention (CDC),
but it is unlikely the virus would spread on a plane unless a passenger
were to come into contact with a sick person's bodily fluids.
The CDC has sent
guidance to American air carriers on how to identify and deal with
passengers displaying Ebola symptoms -- and how they should disinfect
aircraft after an infected passenger leaves a plane.
"Airline carriers, crew
members, and airports can be very important partners in that front
line," Cetron told CNN. "Being educated, knowing the symptoms,
recognizing what to do, having a response protocol, knowing who to call
-- those are really really important parts of the global containment
strategies to deal with threats like this."
Health officials are
also trying to track down everyone who was on any of the three flights
Patrick Sawyer took to get to the heavily populated city of Lagos, in
order to test them for Ebola.
What else is being done to stop the spread of the disease?
Ebola patients are being
isolated by health officials in Western Africa, and those who have come
into contact with them are being told to monitor their temperatures.
The family of a second infected American aid worker had been living with
him in Liberia, but they left before he started showing symptoms. While
it's unlikely they contracted Ebola, the CDC is keeping the family on a
21-day fever watch.
The president of Liberia has
closed most of the borders with neighboring countries,
and the few points of entry that are still open will have Ebola testing
centers. The president also placed restrictions on public gatherings
and ordered hotels, restaurants and other entertainment venues to play a
five-minute video on Ebola safety.
Arik Air, one of
Nigeria's biggest airlines, has also suspended operations into Monrovia
and Freetown, the capitals of Liberia and Sierra Leone, respectively,
according to AllAfrica.com.
The UK government is
also convening an emergency meeting Wednesday to discuss the threat of
Ebola to Britain. There have been no cases of Ebola reported in the UK
as of yet.
The CDC has also issued
an alert to health workers in the U.S. to watch out for any patients who
may have recently traveled to West Africa and could have contracted the
virus.
Why does Ebola generate such fear?
"It is a highly
infectious virus that can kill up to 90% of the people who catch it,
causing terror among infected communities," it says. The death rate in
this outbreak has dropped to roughly 55% because of early treatment.
There is also no vaccination against it.
Of Ebola's five sub-types, the Zaire strain -- the first to be identified -- is considered the most deadly.
The WHO said
preliminary tests on the Ebola virus in Guinea in March suggested that the outbreak there was this strain, although that has not been confirmed.
 Tracking the Ebola virus in Nigeria
Tracking the Ebola virus in Nigeria
 Ebola scientist: 'It's spectacular'
Ebola scientist: 'It's spectacular'
 Ebola epidemic 'out of control'
Ebola epidemic 'out of control'
 Fighting Ebola in urban Africa
Fighting Ebola in urban Africa
What is Ebola?
The Ebola virus causes viral hemorrhagic fever (VHF), which
according to the U.S. Centers for Disease Control and Prevention (CDC), refers to a group of viruses that affect multiple organ systems in the body and are often accompanied by bleeding.
The virus is named after
the Ebola River in the Democratic Republic of Congo (formerly Zaire),
where one of the first outbreaks occurred in 1976. The same year there
was another outbreak in Sudan.
The WHO says there are
five different strains of the virus -- named after the areas they
originated in. Three of these have been associated with large outbreaks
of hemorrhagic fever in Africa.
These are the Bundibugyo -- an area of Uganda where the virus was discovered in 2007 -- Sudan and Zaire sub-types.
There has been a solitary case of Ivory Coast Ebola.
This subtype was discovered when a researcher studying wild chimpanzees became ill in 1994 after an autopsy on one of the animals. The researcher recovered.
Finally, Reston Ebola
is named after Reston in the U.S. state of Virginia, where this fifth strain of the Ebola virus was identified in monkeys imported from the Philippines.
The CDC says while humans have been infected with Ebola Reston, there have been no cases of human illness or death from this sub-type.
What are Ebola's symptoms?
Early symptoms of the
Ebola virus include sudden onset of fever, weakness, muscle pain,
headaches and a sore throat. These symptoms can appear two to 21 days
after infection.
The WHO says these
non-specific early symptoms can be mistaken for signs of diseases such
as malaria, typhoid fever, meningitis or even the plague.
MSF says some patients may also develop a rash, red eyes, hiccups, chest pains and difficulty breathing and swallowing.
The early symptoms
progress to vomiting, diarrhea, impaired kidney and liver function and
sometimes internal and external bleeding.
Ebola can only be definitively confirmed by five different laboratory tests.
How is it treated?
There are no specific treatments for Ebola. MSF says patients are isolated and then supported by health care workers.
"This consists of
hydrating the patient, maintaining their oxygen status and blood
pressure and treating them for any complicating infections," it says.
Carers are advised to
wear impermeable gowns and gloves and to wear facial protection such as
goggles or a medical mask to prevent splashes to the nose, mouth and
eyes.
MSF says it contained a
2012 outbreak in Uganda by placing a control area around its treatment
center. An outbreak is considered over once 42 days -- double the
incubation period of the disease -- have passed without any new cases.
How does it spread?
The WHO says it is
believed that fruit bats may be the natural host of the Ebola virus in
Africa, passing on the virus to other animals.
Humans contract Ebola through contact with the bodily fluids of infected animals.
The WHO says in Africa
there have been documented cases of humans falling ill after contact
with dead or ill chimpanzees, gorillas, fruit bats, monkeys, forest
antelope and porcupines.
It says Ebola later
spreads from human-to-human via contact with bodily fluids containing
the virus. The virus can be spread through contact with an object
contaminated with infected secretions.
Direct contact with the
corpses of Ebola victims can also result in infection and the virus can
be transmitted via infected semen up to seven weeks after clinical
recovery.
MSF says while the virus
is believed to be able to survive for some days in liquid outside an
infected organism, it is fragile and chlorine disinfection, heat, direct
sunlight, soaps and detergents can kill it.
MSF epidemiologist
Kamiliny Kalahne says outbreaks usually spread in areas where hospitals
have poor infection control and limited access to resources such as
running water.
"People who become sick
with it almost always know how they got sick: because they looked after
someone in their family who was very sick -- who had diarrhea, vomiting
and bleeding -- or because they were health staff who had a lot of
contact with a sick patient," she says.
How many cases have there been?
The
CDC estimates there have been more than 1,800 cases of Ebola and more than 1,300 deaths.
The last recorded outbreaks before the current one in Guinea were in 2012 -- in Uganda and Democratic Republic of Congo.
The Uganda outbreak involved a total of 24 probable and confirmed cases, and 17 deaths,
according to the WHO, which declared it had ended in October 2012.
MSF said the Uganda outbreak
had been the Sudan strain, while the virus found in DRC was the Bundibugyo sub-type.
According to the CDC,
the most deadly outbreak was the 1976 outbreak in then Zaire, when 280
of 318 infected people died. In 2000, there were 425 cases of Ebola
Sudan in Uganda, which resulted in 224 fatalities.
 Mark and Priscilla Zuckerberg were the most generous donors in 2013, according to The Chronicle of Philanthropy.Facebook founder Mark Zuckerberg will donate $25 million to combat the outbreak of the deadly Ebola virus.
Mark and Priscilla Zuckerberg were the most generous donors in 2013, according to The Chronicle of Philanthropy.Facebook founder Mark Zuckerberg will donate $25 million to combat the outbreak of the deadly Ebola virus.
 NBC's medical correspondent Dr. Nancy Snyderman has issued an apology after she reportedly violated the quarantine her team was placed in when their cameraman contracted Ebola.
NBC's medical correspondent Dr. Nancy Snyderman has issued an apology after she reportedly violated the quarantine her team was placed in when their cameraman contracted Ebola.


![[ image: The extract can be eaten or rubbed into the skin]](http://news.bbc.co.uk/olmedia/410000/images/_411030_garcinia_kola150.jpg)
![[ image: The Ebola-Zaire virus close up]](http://news.bbc.co.uk/olmedia/410000/images/_411030_ebola_zaire_virus150.jpg)
![[ image: Dr Maurice Iwu said the discovery was a breakthrough]](http://news.bbc.co.uk/olmedia/410000/images/_411030_dr_maurice_iwu150.jpg)
![[ image: Towns are quarantined following an outbreak]](http://news.bbc.co.uk/olmedia/410000/images/_411030_ebola_kids_quarantine150.jpg)